Wearable EEG for Mental Health: What the Evidence Shows
Mental health monitoring has a measurement problem — & EEG is addressing it. From neurofeedback RCTs to real-world stress classification, this piece breaks down where the evidence stands today.
EEG has moved from clinical instrument to field-deployed wearable, achieving 81% stress classification accuracy and outperforming HRV across standardized cognitive stress tasks — expanding the scope of neural monitoring beyond controlled lab conditions.
Mental health care has a fundamental measurement problem. Clinical assessment relies on self-report: structured interviews, standardized questionnaires, patient-disclosed symptom histories. This approach is structurally constrained — memory is selective, self-perception is biased, and symptom disclosure is often delayed by months or years after onset. Electroencephalography (EEG) operates differently. It records the brain's electrical activity directly, continuously, and without requiring the patient to interpret or communicate their internal state.
Why EEG Among Non-Invasive Neuroimaging Options
The four primary non-invasive neuroimaging modalities differ significantly in practical and technical profile:
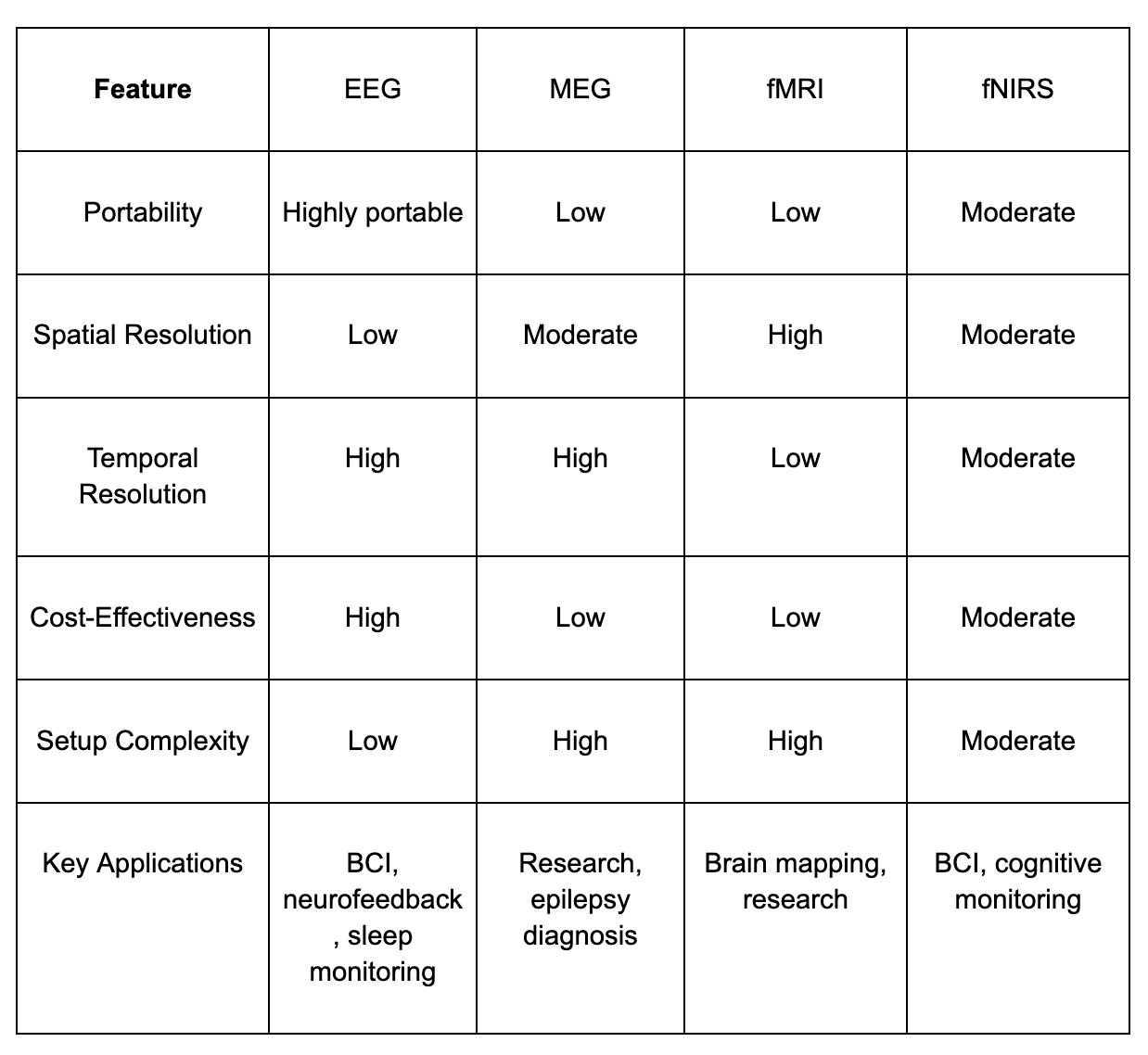
For mental health monitoring, EEG's combination of high temporal resolution, portability, and low setup complexity makes it the most viable option for real-world deployment. Its primary limitation — susceptibility to noise and lower spatial resolution — is being progressively mitigated through modern signal processing and machine learning.
EEG signal types relevant to mental health
EEG captures electrical activity across five frequency bands, each associated with distinct cognitive states:
- Delta (0.5–4 Hz): Deep sleep; disrupted patterns observed in depression and TBI.
- Theta (4–8 Hz): Memory encoding and emotional processing; elevated frontal theta associated with anxiety and cognitive load.
- Alpha (8–13 Hz): Relaxed wakefulness; suppression is a consistent marker of stress and heightened arousal.
- Beta (13–30 Hz): Active thinking and focused attention; elevated beta is the primary neural signature of stress and anxiety.
- Gamma (30–100 Hz): Higher cognitive functions; relevant to attention and working memory research.
The alpha-beta relationship is particularly informative — stress consistently produces increased beta power alongside suppressed alpha rhythms, a pattern detectable in ambulatory settings across real-world stressors.
From passive monitoring to neurofeedback
EEG's most clinically validated mental health application is neurofeedback — a therapeutic modality in which patients modulate their own brain activity through real-time audio or visual feedback derived from their EEG signal. Unlike pharmacological or cognitive-behavioral approaches, neurofeedback uses the brain's own electrical output as the training signal.
Across 14 randomized controlled trials involving 718 participants with ADHD, EEG neurofeedback produced statistically significant improvement in sustained attention, with the strongest outcomes in beta wave enhancement protocols.[2] A 2025 meta-analysis of 17 RCTs in children and adolescents confirmed measurable gains in executive function, though standardized protocols remain a prerequisite for broader clinical adoption.
EEG vs. HRV: Stress classification accuracy
HRV has been the dominant biometric proxy for stress in consumer and clinical wearables. Researchers at A*STAR institute conducted a direct comparison on identical cognitive stress tasks: EEG-based classification achieved 81% accuracy versus 56–62% for HRV models. HRV measures downstream autonomic activity; EEG captures the cortical changes that precede and drive those autonomic responses — the alpha suppression and beta elevation that characterize stress at its neural source.
Deep learning architectures have extended this further. Recent Studies demonstrated 92.5% classification accuracy across multiple mental health datasets, with an AUC of 94.2% — performance attributable to transformer-based architectures and individualized baseline modeling.
Burnout: From subjective profile to neural marker
Burnout is currently assessed through the Maslach Burnout Inventory — entirely self-reported. EEG research identifies reduced P300 amplitude as a quantifiable neural correlate. The P300 is an event-related potential associated with attention allocation and cognitive resource availability; its suppression indicates a measurable reduction in the brain's attentional processing capacity. This provides an objective neural indicator of a condition previously defined only through subjective report, and enables longitudinal monitoring prior to clinical symptom onset.
Real-World Deployment: Defense, Sports, and AR/VR
EEG's transition from laboratory to field is driven by dry-electrode wearable design, miniaturized amplification, and on-device processing:
Defense: U.S. Army research programs are evaluating wearable EEG for real-time monitoring of vigilance, cognitive load, and TBI risk in operational environments.The global military wearable sensors market is projected to grow from $0.92B in 2024 to $2.62B by 2033.
Combat Sports: EEG-powered transformer models are tracking neural state across ~650 athletes in combat sports, mapping how high-contact participation shapes brain function over time — relevant to both performance optimization and longitudinal neural impact assessment.
AR/VR: EEG integration enables real-time classification of attention state and cognitive fatigue during immersive training and rehabilitation, with closed-loop systems — where a detected cognitive state triggers an environmental adjustment — actively under development.
The Individual Calibration Problem
The primary unresolved challenge is inter-individual variability. Population-level neural markers do not reliably map to individual baselines — a beta power level indicating stress in one individual may represent normal resting state in another. The research response is personalized adaptive modeling: establishing an individual-specific neural baseline, then classifying deviations from it. Consumer-grade dry-electrode EEG wearables combined with on-device ML make this technically feasible; the barrier is accumulating sufficient longitudinal individual-level data to distinguish signal from noise.
Neural Data: Governance considerations
EEG is a direct readout of cognitive and emotional state — capturing attention, arousal, and mental load at a resolution with no precedent in consumer health monitoring. As EEG systems move toward real-world deployment, they require robust data protection protocols, transparent consent frameworks, and defined user control over neural data. The current regulatory environment has not kept pace with the deployment trajectory of EEG wearables. Closing that gap in parallel with technical development — not after — is a necessary condition for responsible scaling.
Current Evidence: What EEG supports & what remains open
Supported by current evidence:
- Stress classification at 81% accuracy in wearable settings, outperforming HRV by 20+ percentage points
- Deep learning EEG classification at 92.5% accuracy across mental health datasets (AUC 94.2%)
- Neurofeedback producing measurable attention improvement across 14 RCTs in ADHD
- Neurofeedback improving executive function across 17 RCTs in children and adolescents
- P300 suppression as a quantifiable neural correlate of burnout
- Wearable EEG validated in defense, combat sports, and immersive training environments
Requiring further development:
- Individual-level validation across diverse populations
- Standardized neurofeedback protocols for clinical adoption
- Longitudinal data infrastructure for personalized baseline modeling
- Regulatory frameworks for neural data collection outside research settings
The signals are measurable, the hardware is field-deployable, and classification models have reached clinically meaningful performance thresholds. Whether that translates into reliable clinical utility depends on the validation, standardization, and governance work still ahead
Sources:
[1] NAMI — Mental Health By the Numbers. nami.org
[2] Chiu et al. (2022) — PMC9764556
[3] Zhong et al. (2025) — Scientific Reports, 15: 28148
[4] NeuroSci (2024) — DOI: 10.3390/neurosci5040031
[5] RTI Press (2024) — ncbi.nlm.nih.gov/books/NBK602203
[6] SkyQuestt (2025) — skyquestt.com
[7] PMC (2025) — PMC12194295
[8] Liu & Zhao (2025) — DOI: 10.3389/fninf.2024.1494970
Further reading


Subscribe to Neurotech Pulse
A roundup of the latest in neurotech covering breakthroughs, products, trials, funding, approvals, and industry trends straight to your inbox.